Compared to endometriosis, adenomyosis (pronounced ad-en-oh-my-o-sis) is a little-known and under-researched condition: endometriosis’ poor cousin. However, ‘adeno’ is an important condition, which often causes heavy and painful periods. It can have a range of impacts on a woman’s life: from the monthly annoyance of heavy and painful periods, to big life choices (especially about having children). Read on for a basic primer on all things adenomyosis…
What is adenomyosis?
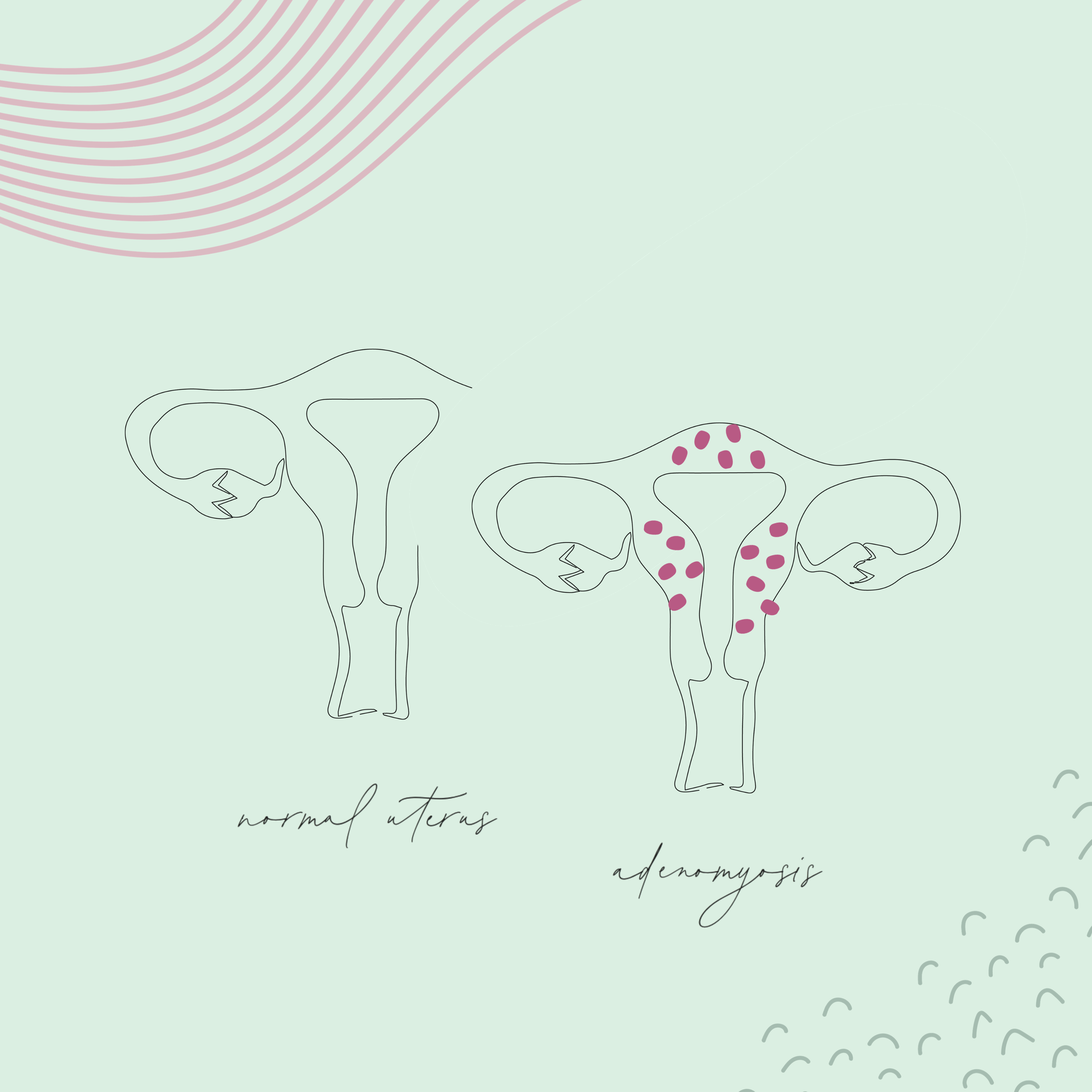
Adenomyosis is a benign condition, in which the lining of the uterus (called the ‘endometrium’) grows a little bit too deeply, into the muscle of the uterus (the ‘myometrium’).
To understand adenomyosis, you have to understand how the endometrium (the uterine lining) works. The endometrium is a special type of glandular tissue, that responds to the monthly fluctuations in a woman’s hormones. Every month during a woman’s reproductive life (from the day of your first period, to the day of your last), the endometrium: gets thicker to prepare for a pregnancy, then (if a pregnancy doesn’t happen), it sloughs off (rather like a snake shedding its skin) during your period.
In adenomyosis, some of these endometrial glands grow a little too deeply, into the myometrium (the muscle of the uterus). These glands still respond to the monthly hormonal fluctuations: hence, they swell and get bigger for three weeks a month, then bleed during a woman’s period.
What causes adenomyosis?
Experts aren’t exactly sure what causes adenomyosis, but risk factors may include:
- Age: Most women with adenomyosis are in their later childbearing years, between 35 and 50yo. Most symptoms of adenomyosis dissipate after menopause.
- Childbirth: Many women with adenomyosis have given birth to more than one child. Endometrial tissue could invade the myometrium when an embryo implants in the uterine wall. But the fact that women tend to accumulate children as they age may be a confounding factor here…
- Previous surgeries: Some studies suggest that prior uterine surgeries (e.g. Caesarean section, or a dilation and curettage), could make adenomyosis more likely.
How common is adenomyosis?
Strictly speaking, adenomyosis can only be definitively diagnosed after a woman’s uterus is removed (e.g. at a hysterectomy operation) and looked at under a microscope by a pathologist. Hence, there are many women walking around with adenomyosis, who haven’t yet been diagnosed, and it’s hard to guess what percentage of women have adenomyosis. That’s largely why estimated vary widely, from 5% to 70%. Approximately 25% of uteruses are that are removed surgically (at hysterectomy) have adenomyosis. ‘Adeno’ is a common cause of problematic heavy and painful periods.
While adenomyosis can affect a woman of any age, it does tend to get worse with age, up until menopause.
What symptoms does adenomyosis cause?
Adenomyosis often causes heavy menstrual bleeding. Normally, the periods of a woman who has adenomyosis are manageable until their mid to late 30s, then get increasingly heavy over time (throughout their 40s). Adenomyosis also causes painful periods: just like the heaviness of bleeding, period pain due to adenomyosis often gets worse with age, up until menopause.
Adenomyosis often causes the uterus to be bigger than usual, which can lead to a sense of abdominal distension and constant bloating. There may also be a sense of pelvic heaviness or fullness.
How is adenomyosis diagnosed?
If a doctor examines you, they may find that your uterus is bigger than usual. This is one hint that you may have adenomyosis.
The next step towards diagnosing adenomyosis is a transvaginal ultrasound. Suggestive findings at ultrasound include:
- A big (or ‘bulky’) uterus, which may be described as ‘globular’
- One particular side of the uterus being thicker than the other (e.g. the back wall thicker than the front wall)
- A ‘streaky’ or inconsistent texture to the uterine muscle, which may be described as ‘heterogeneous’
- A pattern of shadowing called ‘Venetian blinds’
If a pelvic MRI is ordered for some reason, adenomyosis may be diagnosed: MRI provides incredibly high-resolution images of the uterus.
While adenomyosis may be suspected based on a patient’s symptoms, ultrasound or MRI findings, it can only be definitively diagnosed when the uterus is analysed by a pathologist using a microscope (i.e. after a hysterectomy).
How is adenomyosis treated?
Broadly speaking, there are several management approaches for adenomyosis: symptomatic relief; hormonal suppression; and surgical excision. Women with mild symptoms may choose to manage their ‘adeno’ with medicines, while awaiting menopause. Women who have completed their families, with moderate to severe symptoms, may want a hysterectomy.
Symptomatic relief
The main symptoms of adenomyosis (principally heavy and painful periods) can be managed using the following approaches:
- Simple pain relief, such as paracetamol and ibuprofen or naprogesic
- Tranexamic acid and / or mefenamic acid tablets, taken during your period
- Iron supplements, in the form of tablets or an iron infusion
Hormonal suppression
Hormonal medications such as the contraceptive Pill can help manage symptoms to some extent, in that The Pill lightens periods and helps to lessen period pain. The progesterone-containing intra-uterine device (called ‘Mirena’) may also help to lighten your periods.
However, neither The Pill nor Mirena will shrink down a uterus that is bulky due to adenomyosis. Hence, any so-called ‘pressure symptoms’ (such as pelvic heaviness or dragging, abdominal bloating, and lower back pain) will remain.
Surgical excision
The only definitive management for adenomyosis is hysterectomy: an operation to remove the uterus. As this removes the cause of the adenomyosis, it is guaranteed to treat any heavy menstrual bleeding: once the uterus has been removed, you will not have any regular monthly bleeding.
Removing the uterus should also completely treat any adenomyosis-related period pain, but there is no guarantee. If you have any additional causes of pelvic pain (such as endometriosis), this will need to be treated at the same time (e.g. excised during the same keyhole surgery operation at which the hysterectomy is performed).
Surgical excision also allows the diagnosis to be made definitively, in that the uterus can be sent to the laboratory for the pathology doctors to examine under a microscope, thereby confirming the suspected diagnosis.
Conclusion
Adenomyosis is a common cause of both heavy and painful periods, amongst women in their mid-30s to 50s. While it is not cancerous, the symptoms it causes can significantly impact upon women’s quality of life. While medications can be taken to try to manage the related symptoms, hysterectomy is the best approach for definitive diagnosis and treatment.
Frequently asked questions (FAQs)
What should I do if I have suspected adenomyosis, but am trying to conceive?
You can try the approaches listed above for symptomatic relief, such as: tranexamic acid; mefenamic acid; over-the-counter pain relief; and iron supplementation. Unfortunately all of the hormonal management options are also contraceptive, so can’t be used if you’re trying to conceive. Obviously hysterectomy precludes future pregnancy.
Can you remove the adenomyosis without removing the whole uterus?
Generally, adenomyosis causes diffuse projections of endometrial tissue that invade into the muscle of the uterus, throughout the whole uterus. Sometimes, an ultrasound report mentions ‘focal’ adenomyosis – i.e. adenomyosis just in one distinct area of the uterine muscle. In other parts of the world (e.g. Europe), some gynaecologists have attempted an ‘adenomyomectomy’ operation, in which just the affected area of uterine muscle is removed. The remaining uterine muscle is then stitched together, and pregnancy attempted. This is an investigational approach: even when performed by the best of surgeons, there is a risk of uterine rupture in future pregnancies. There is very limited evidence to support this approach, and no gynaecologists in Australia perform this operation.
Is ‘endometrial ablation’ an option to treat adenomyosis?
Endometrial ablation is a day procedure (performed under general anaesthetic) in which the lining of the uterus is burnt. While ablation destroys the lining of the uterus, and may help somewhat with heavy periods, it doesn’t cause the underlying problem. Hence, ablation is less likely to be successful in women with adenomyosis, compared to women with heavy periods who don’t have adenomyosis.