An ectopic pregnancy is a serious condition, that affects around 2% of all pregnancies. It occurs when an early embryo (or ‘blastocyst’) implants outside the uterus: the vast majority of the time, in the Fallopian tube. While uncommon, ectopic pregnancy is the most dangerous cause of pain and bleeding in early pregnancy, and is a leading cause of maternal death in the first trimester globally.
That sounds frightening, but knowledge is power! Early diagnosis and prompt treatment save lives, and also helps to preserve fertility. In this blog, we’ll walk through what ectopic pregnancy is, the symptoms to watch for, how it’s diagnosed and treated, and what the future implications are.
What is an ectopic pregnancy?
In a healthy pregnancy, the early embryo travels down the Fallopian tube, and implants in the lining of the uterus. In an ectopic pregnancy, implantation happens outside the uterus: most commonly in a Fallopian tube, but sometimes on the ovary, in the cervical canal, or even the abdominal cavity.
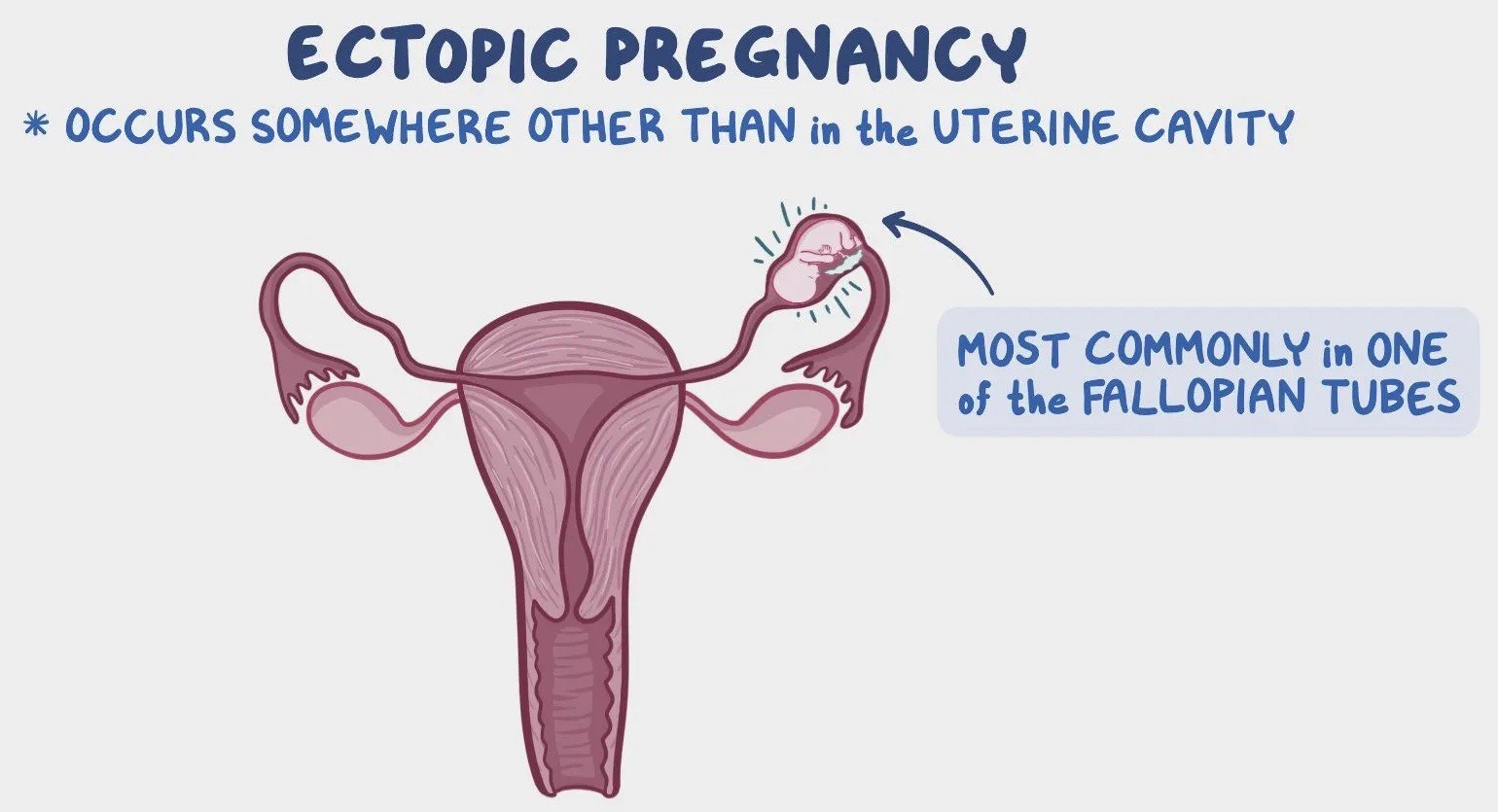
[ Source: www.osmosis.org/learn/Ectopic_pregnancy:_Nursing ]
Unfortunately, an ectopic pregnancy will never develop into a healthy baby, as there is not enough space to grow safely without impacting on the mother’s life. If left untreated, it can cause the affected Fallopian tube to rupture, leading to internal bleeding and a life-threatening emergency for the mother.
Who’s at risk?
Ectopic pregnancy occurs in about 1 in 50 (or 2% of) pregnancies. Risk factors include:
- Previous ectopic pregnancy: risk of recurrence is five-fold (about 10%)
- Damage to Fallopian tubes, due to previously pelvic infection, tubal surgery, or endometriosis
- In vitro fertilisation (IVF) conception
- A progesterone intrauterine device (IUD) in place at the time of conception. Progesterone IUDs prevent 99.9% of pregnancies. But if you happen to be in the 0.1% of women who conceive with a progesterone IUD in place, there is a 50% chance that the resultant embryo will implant and grow in a Fallopian tube
- Maternal age over 35yo
It’s important to note that about half of women who experience ectopic pregnancy have no identifiable risk factors. That’s why any pain or bleeding in early pregnancy should be carefully assessed by your woman’s health GP, in collaboration with the early pregnancy assessment service at your local maternity hospital.
Symptoms: what to look out for
Ectopic pregnancy often starts with the same symptoms as a normal pregnancy: a missed period, a positive urine pregnancy test, breast tenderness, and nausea. But as an ectopic pregnancy progresses, certain warning signs may develop, including:
- Abdominal or pelvic pain (often on one side, sometimes sharp, often persistent)
- Vaginal bleeding or spotting
- Shoulder tip pain (which is a sign of internal bleeding irritating the diaphragm)
- Dizziness, fainting, or collapse (which is suggestive of tubal rupture and significant internal bleeding)
Around 80% of ectopic pregnancies are diagnosed before tubal rupture, but in 20% of cases, the first sign may be sudden severe pain and collapse.
If you are pregnant and experience these symptoms (especially sudden severe pain or dizziness), seek urgent medical care immediately, at your local maternity hospital Emergency Department if needs be.
How ectopic pregnancy is diagnosed
Doctors use a combination of:
- Pregnancy hormone (BhCG) levels on repeated blood tests: in a healthy early pregnancy, BhCG should rise by at least 50% every 48 hours. In ectopic pregnancies, it often rises more slowly, plateaus, or falls.
- Transvaginal ultrasound: this is the key investigation. Sometimes the ectopic sac itself is visible in a Fallopian tube on ultrasound scan.
- Clinical examination and assessment: pain, tenderness, and bleeding patterns all guide the diagnosis.
Treatment options
Management depends on your condition (i.e. whether you have significant internal bleeding or not), the size of the developing pregnancy on ultrasound, and your BhCG hormone level on blood tests.
Expectant, or ‘watch-and-wait’
Sometimes, an ectopic pregnancy resolves on its own. If the pregnancy is very small, BhCG levels are low and falling, and you are stable, close monitoring with repeat blood tests with / without repeated ultrasounds may be a safe option.
Medical: methotrexate injection(s)
If your ectopic pregnancy is small, unruptured, and BhCG levels are below about 5000IU/L, a medication called methotrexate may be given, by intramuscular injection (similar to a vaccination). This stops the pregnancy cells from growing, allowing the body to absorb the tissue. This will be done under the guidance of your local maternity hospital’s early pregnancy assessment service, and requires close follow-up with repeated blood tests. Because methotrexate is a chemotherapy medication, it’s important that you don’t conceive within 3 months of having it.
Surgical: keyhole surgery to remove the affected Fallopian tube
Surgery is required if the ectopic pregnancy is large, BhCG levels are high, there is a fetal heartbeat, and / or you are in pain or unstable. This is usually done via laparoscopy (keyhole surgery) to remove the pregnancy and the affected Fallopian tube: a procedure called ‘laparoscopic salpingectomy’.
In emergency cases of tubal rupture and significant internal bleeding, urgent surgery is life-saving.
What about future fertility?
Understandably, one of the biggest concerns for women after an ectopic pregnancy is: “Will I be able to have children in the future?”
- If one tube is removed, the other can often still function normally, so natural conception is likely
- The risk of another ectopic pregnancy is around 10%, regardless of how your ectopic pregnancy was treated (expected, medical, or surgical management)
- Very occasionally, a woman may have had two tubal ectopic pregnancies, both of which required surgical removal of the affected Fallopian tube. In these situations, you won’t be able to conceive naturally, and will need IVF to conceive in future
In all future pregnancies, an early ultrasound scan (at around 6 weeks’ gestation) is essential, to confirm the next embryo is growing in the uterus (where it should be!)
Emotional impact
Beyond the physical aspects, ectopic pregnancy is often an emotionally traumatic experience. Many women (and their partners) grieve the loss of a much-wanted pregnancy, while also dealing with fear for their health. Feelings of sadness, anger, and anxiety are all common.
Support is available through organisations such as the UK’s The Ectopic Pregnancy Trust, or Red Nose Australia. Speaking to your women’s health GP, gynaecologist, or a counsellor can also be very helpful.
Key takeaways
- Ectopic pregnancy affects about 1 in 50 pregnancies
- Any early pregnancy with pain or bleeding should be assessed at your local maternity hospital, as ectopic pregnancy must be excluded
- Diagnosis is made with BhCG blood tests and a transvaginal ultrasound
- Treatment may be expectant, medical, or surgical, depending on the situation
- Future fertility is often preserved, but early scans are important in subsequent pregnancies
- The emotional impact is real, so emotional support is vital
Conclusions
Ectopic pregnancy can sound frightening, but with early recognition and prompt management, outcomes are usually very good. The most important thing is to seek medical advice quickly if you are pregnant and have pain and / or bleeding.
If you have concerns about your risk, your symptoms, or what an ectopic pregnancy might mean for your future, please see your woman’s health GP (such as Maven Centre’s Dr Amy Sinclair-Thomson or Dr Phillippa Wooton) or a gynaecologist. At Maven Centre, we are here to provide expert, compassionate care every step of the way.