Endometriosis surgery is often described as both an art and a science — and a large part of that comes down to anatomy.
When performing laparoscopic excision of endometriosis, gynaecological surgeons are not simply ‘burning off spots’ of disease. Instead, they are carefully navigating a dense and complex network of organs, nerves, blood vessels, ligaments, and spaces within the pelvis. Understanding this anatomy is critical for both safe surgery and effective removal of disease.
In this blog, we’ll explore: the key pelvic anatomy involved in laparoscopic endometriosis surgery; why endometriosis can affect so many different organs; and how anatomical knowledge helps advanced gynaecological surgeons such as Dr Alison Bryant-Smith and Dr Sneha Parghi perform precise and fertility-preserving operations.
Why Surgical Anatomy Matters so much in Endometriosis Surgery
Endometriosis is a condition in which tissue similar to the lining of the uterus (the ‘endometrium’) grows outside the uterus. While some lesions are superficial (shallow), others can infiltrate deeply into the pelvis and involve nearby structures (so-called ‘deeply infiltrative endometriosis’, or DIE). This means endometriosis surgery is rarely limited to one organ alone.
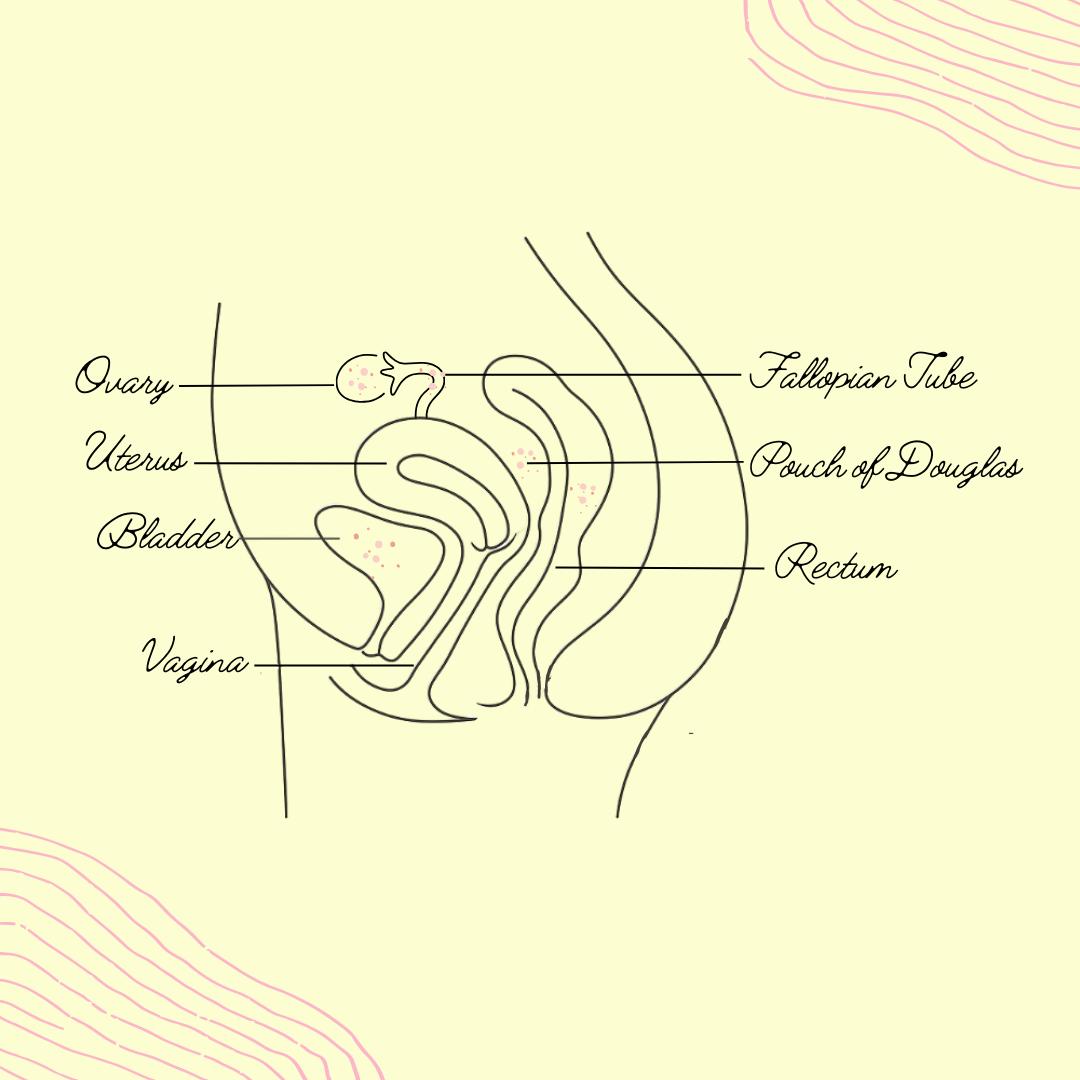
The pelvis is a compact anatomical space where many structures sit close together, including the:
- Uterus (or ‘womb’)
- Cervix
- Ovaries
- Fallopian tubes
- Bowel (esp. the large intestine, which includes the sigmoid and rectum)
- Bladder
- Ureters
- Nerves
- Blood vessels
A surgeon performing laparoscopic excision of endometriosis must therefore understand not only where endometriosis is visible, but also how to safely separate and preserve surrounding vital structures (such as the ureters).
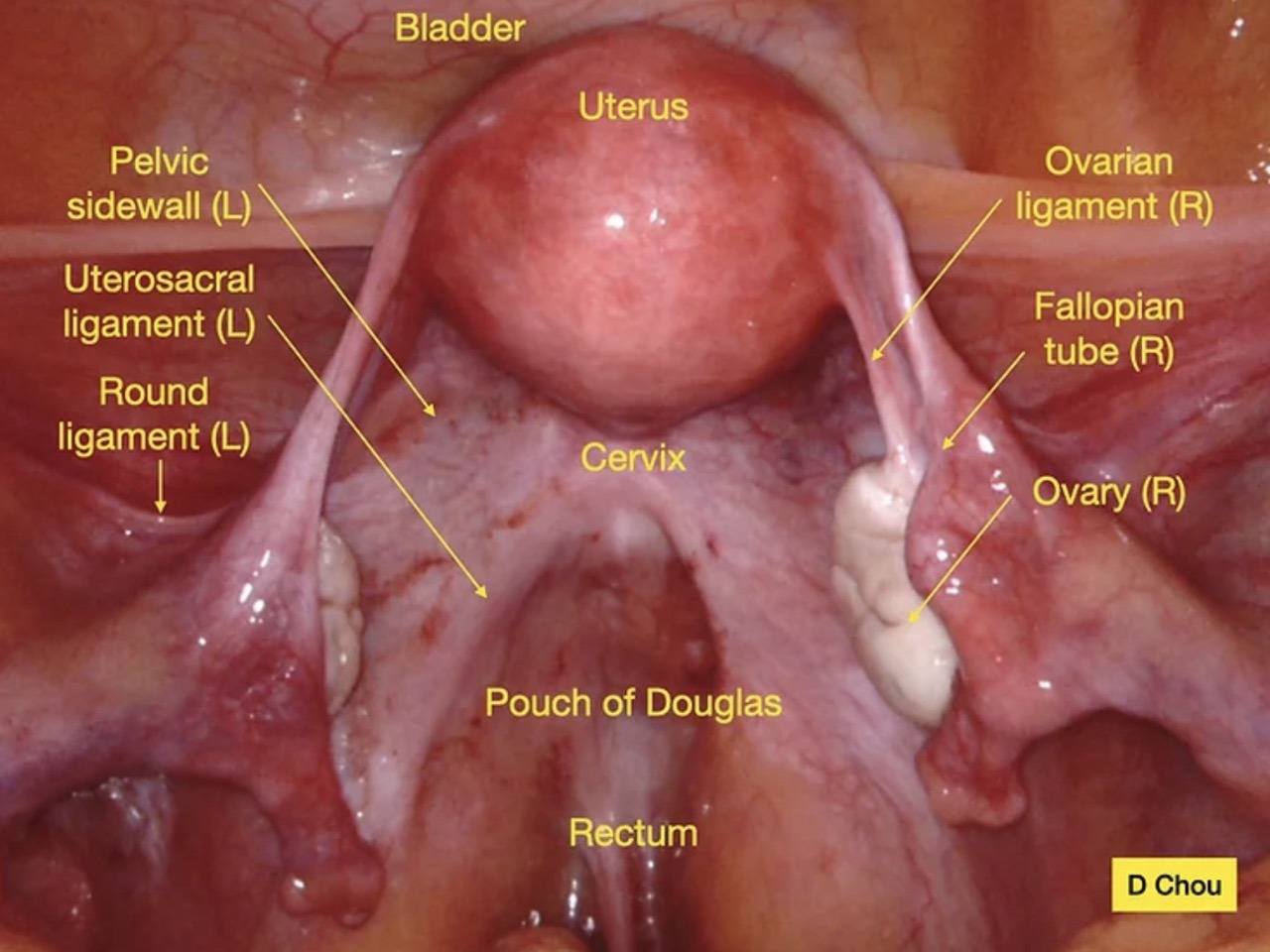
(Keyhole surgery screenshot from Endometriosis Australia website https://endometriosisaustralia.org/anatomy-101-for-surgical-removal-of-endometriosis/ , with thanks to Dr Danny Chou and colleagues.)
A Pelvic Anatomy Refresher
The Uterus
The uterus (0r ‘womb’) sits centrally within the pelvis, between the bladder at the front and the rectum at the back. Several important structures attach to it, including:
- The Fallopian tubes
- The ovaries
- Supporting ligaments (such as the ‘uterosacral ligaments’ and ’round ligaments’)
- Surrounding pelvic connective tissue (such as the ‘broad ligament’)
- Endometriosis commonly develops behind the uterus, particularly in the so-called ‘Pouch of Douglas’
The Ovaries
The ovaries sit on either side of the uterus and are among the most common sites affected by endometriosis. They are attached to the side of the uterus by the ‘ovarian ligament’.
Endometriosis involving the ovaries may form:
- Superficial (shallow) deposits
- Scar tissue (or ‘adhesions’)
- Ovarian cysts called endometriomas ( or ‘chocolate cysts’)
- Because the ovaries are closely related to the pelvic sidewall, ureters, and bowel, surgery in this area requires meticulous dissection
Preserving healthy ovarian tissue is especially important in patients wishing to optimise fertility. The keyhole surgery photos show robotic excision of a left ovarian endometriotic cyst:
(A) The enlarged left ovary, due to an endometriotic cyst
(B) The ‘endometrioma’ being shelled out from the inside of the normal left ovarian tissue
(C) The endometrioma (on the left) being stripped out of the left ovarian tissue (on the right), which is now opened out and displayed
(D) The left ovary after it has been stitched (‘sutured’) closed again
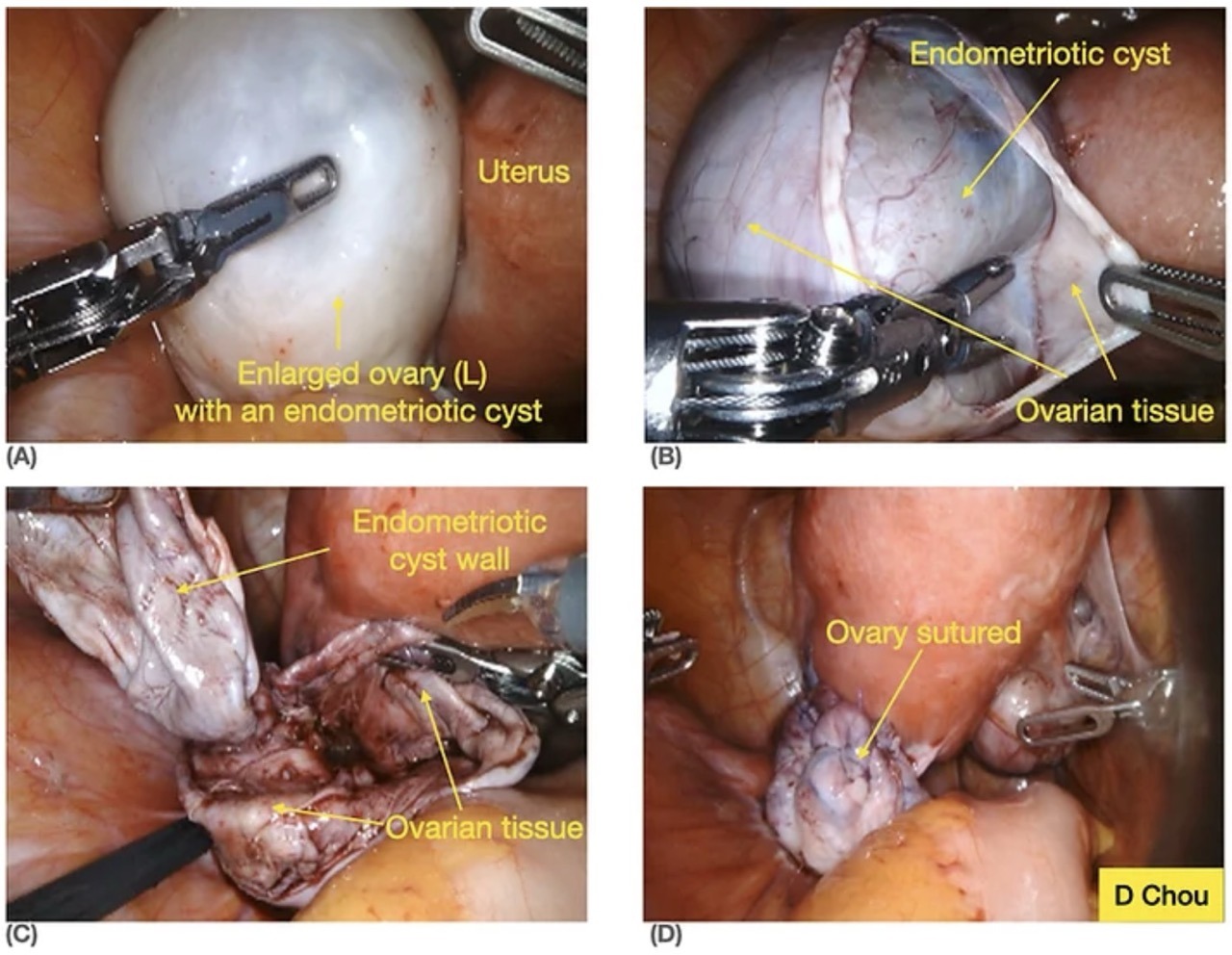
(Keyhole surgery screenshot from Endometriosis Australia website https://endometriosisaustralia.org/anatomy-101-for-surgical-removal-of-endometriosis/ , with thanks to Dr Danny Chou and colleagues.)
The Fallopian Tubes
The Fallopian tubes connect the ovaries to the uterus and are essential for natural conception. Endometriosis may:
- Distort the tubes
- Tether them with scar tissue
- Impair their mobility (or movement)
- Contribute to infertility
Part of laparoscopic excision surgery often involves restoring normal pelvic anatomy and freeing ‘adhesions’ (internal scarring) around the tubes and ovaries.
The “Pouch of Douglas”: a common site for endometriosis
One of the most important anatomical areas in endometriosis surgery is the Pouch of Douglas: an area where endometriosis often develops. This is the space between:
- The uterus, cervix and vagina at the front
- And the rectum at the back
It is one of the most common sites for ‘deeply infiltrating endometriosis’ (DIE). Disease here can cause:
- Severe period pain
- Pain during intercourse
- Painful bowel motions
- Cyclical bowel symptoms (eg. constipation prior to your period, then diarrhoea during your period)
- In advanced cases, scar tissue can completely ‘obliterate’ this space, binding the bowel, uterus, and surrounding organs together, as if with glue.
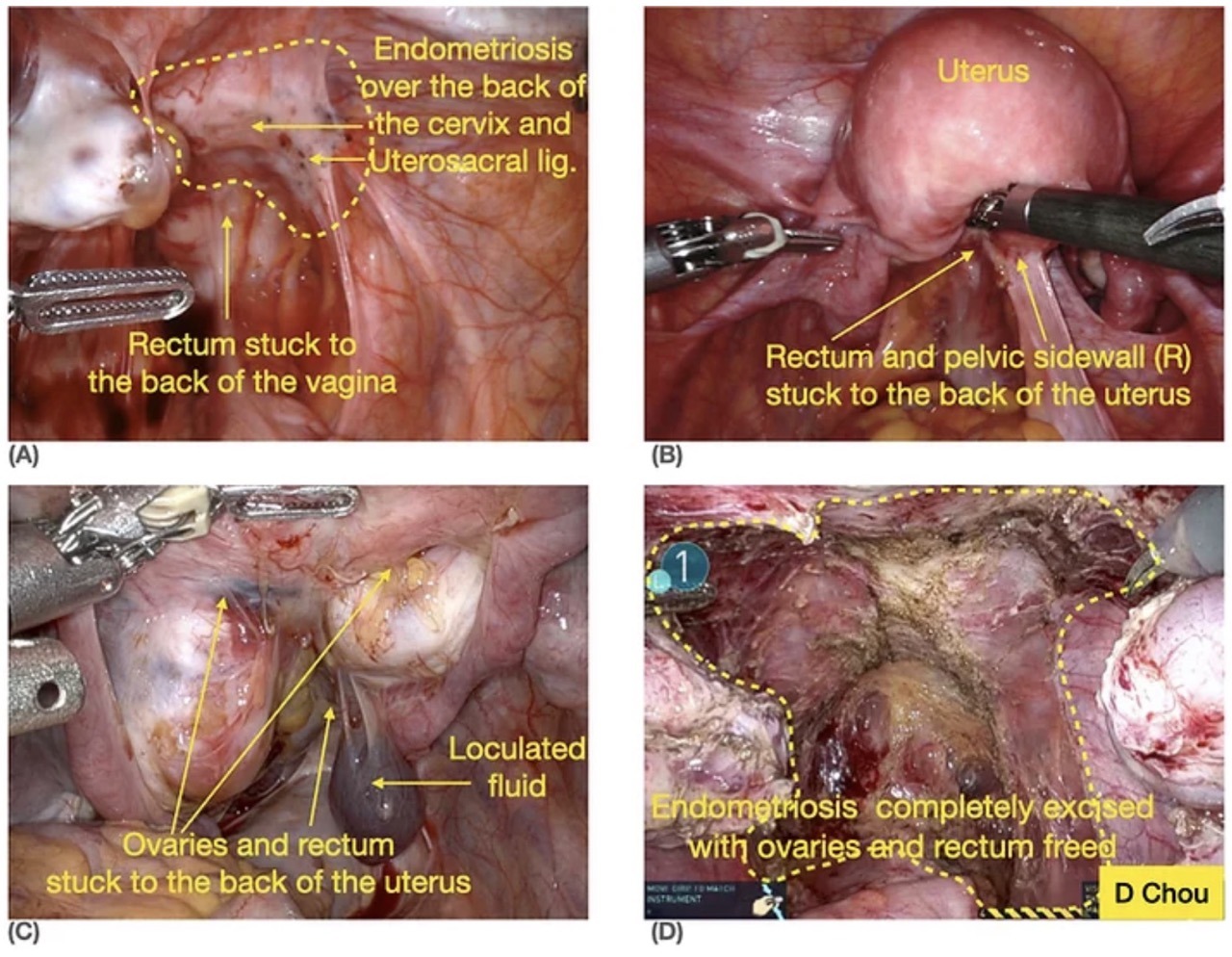
(Keyhole surgery screenshot from Endometriosis Australia website https://endometriosisaustralia.org/anatomy-101-for-surgical-removal-of-endometriosis/ , with thanks to Dr Danny Chou and colleagues.)
Restoring this anatomy laparoscopically is often one of the most technically demanding parts of advanced endometriosis surgery.
The Bowel
Endometriosis can involve the bowel in more severe cases, most commonly:
- Sigmoid colon
- The rectum (the penultimate part of the large intestine, before faeces exits the body via the anus)
When disease infiltrates the bowel wall, symptoms may include:
- Painful bowel motions
- Constipation or diarrhoea
- Cyclical bowel symptoms
Bowel surgery requires particularly detailed anatomical knowledge because the surgeon must preserve:
- Bowel’s blood supply
- Bowel’s nerves
- Surrounding pelvic structures
This is one reason why expert colorectal surgeons (such as Maven Centre’s Dr Fiona Reid) are sometimes involved in advanced endometriosis surgery. This recent blog discusses the role of an endometriosis colorectal surgeon in more detail.
The Bladder and Ureters
The bladder sits directly in front of the uterus. Endometriosis affecting the bladder may cause:
- Urinary urgency
- Pain when the bladder is full
- Cyclical urinary symptoms
- Nearby are the ureters (the thin tubes carrying urine from the kidneys to the bladder)
The ureters run deep within the pelvis and are particularly important during endometriosis surgery because they:
- Can become trapped in scar tissue
- May be pushed away by endometriosis
- They are vulnerable to injury if anatomy is distorted
- One of the key goals of advanced laparoscopic surgery is identifying and protecting the ureters throughout the procedure
Pelvic Sidewalls and Retroperitoneal Spaces
One of the most fascinating aspects of laparoscopic endometriosis surgery is that much of the surgery occurs beneath the surface. Experienced surgeons often work within anatomical “spaces” in the pelvis, including:
- Para-rectal spaces
- Para-vesical spaces
- Retroperitoneal spaces
Developing these spaces allows surgeons to: safely separate organs; identify nerves and the ureters; and to remove deep disease precisely, without causing inadvertent damage to underlying vital structures. The photo below demonstrates brown / black endometriotic nodules that are often seen involving the pelvic peritoneum (the cell layer that lines the inside surface of the abdominal wall and pelvis).
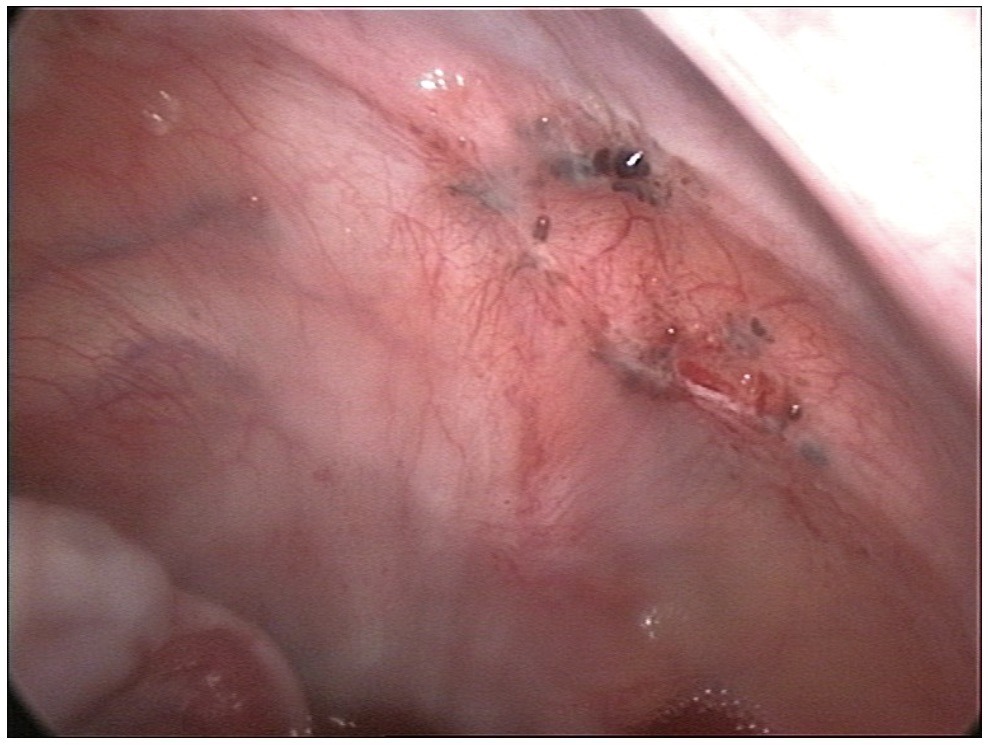
(Keyhole surgery screenshot from https://thecommonvein.com/AshleyDavidoffMD/anatomy-of-endometriosis-and-adenomyosis/ )
Adhesions: when anatomy becomes distorted
Endometriosis causes inflammation, and inflammation leads to scar tissue formation. This internal scar tissue (called ‘adhesions’) can: pull organs out of their normal positions; tether structures together; and distort normal anatomy. For example:
- Ovaries may stick to the pelvic sidewall
- Bowel may adhere to the uterus
- Fallopian tubes may become twisted or trapped
In severe endometriosis, anatomy can become so distorted that surgery resembles reconstructive pelvic surgery. Part of advanced endometriosis surgery involves carefully restoring normal anatomy, while preserving organ function.
Why Laparoscopy Is So Valuable
Compared to traditional (open) surgery, a keyhole surgery (laparoscopic) approach provides: magnified visualisation; high-definition imaging; and excellent access to deep pelvic spaces. This magnification allows surgeons to more easily identify:
- Tiny endometriosis lesions
- Delicate blood vessels
- Pelvic nerves
- Ureters
- ‘Planes’ (or natural seams) between organs
Compared with open surgery, laparoscopy often results in: smaller incisions; less pain; faster recovery; and fewer adhesions. Importantly, it also allows the detailed anatomical dissection required for complex endometriosis surgery.
The Importance of Precision Surgery
Endometriosis surgery is not simply about removing visible disease. It also entails:
- Optimising fertility
- Preserving pelvic organs
- Maintaining bladder and bowel function
- Reducing pain
- Minimising recurrence
This is why many patients with severe disease benefit from gynaecological surgeons with specialised expertise in advanced laparoscopic anatomy and excision techniques.
Final Thoughts
The pelvis is an intricate and tightly packed anatomical space — and endometriosis can affect nearly every part of it. Successful laparoscopic excision of severe endometriosis demands a detailed understanding of pelvic anatomy, careful surgical technique, and a tailored approach to each patient’s disease. For patients, understanding a little of this anatomy can also help explain:
- Why symptoms vary
- Why surgery can be complex
- Why multidisciplinary care is sometimes needed
- And why specialised surgical expertise matters
If you have endometriosis symptoms or are considering surgery, speak with your GP or gynaecologist about whether referral to an experienced laparoscopic endometriosis surgeon (such as those at Maven Centre) may be appropriate for you.